This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Could be FHIR resources, but more likely a database structure specific to the needs of the lab domain. Well, the simple explanation is that it is a FHIR server (in that it exposes a FHIR interface) that specializes in terminology functionality. FHIR Operation? Now this is of course an application specific solution.
This could translate into the health IT customer demanding the use of standards such as FHIR, to enable greater interoperability and appification of the EHR (my word).This We have to start using these standards like FHIR, which part of our evolving toward more open, flexible systems. This is one of my books messages, Harm said.
FHIR DevDays Amsterdam/Europe edition is coming up soon: November 17-20. And, of course, it’s in the european timezone, though there’s also a session specially scheduled for a friendly time in Asia/Pac. No, I want to raise the profile of the special discount that arrangements for the lower/middle income countries.
My tutorial is "FHIR Security and Privacy (TH15)" Not Hacking Unfortunately I did not provide a description for my tutorial, so what is published in the HL7 tutorial guide is based on a previous tutorial. That tutorial was more focused on hacking a FHIR Server. My tutorial is Thursday morning, covering two quarters, about 3 hours.
The FHIR community is not immune to all this; the pandemic means that we’ve had to suspend our regular meeting cycles, and it seems like it will be at least the rest of the year, or even longer, before we can plan to meet face to face again (and even longer for international travel). John Loonsk will present about eCR Now.
It’s a common thing for implementers to want to do with FHIR: connect to a FHIR server, and make a local copy of the information provided by the server, and then check back occasionally with the server for updates – that is, new resources, or changes to existing resources. (In And so the client should also delete it?
The FHIR Standard doesn’t say much about security. There are, however, many different valid approaches to making a server secure, so the FHIR standard delegates making rules about security to other specifications such as the Smart App Launch Specification. Between the client and server. A security appliance is not enough.
On a forum for FHIR Foundation members, I raised the subject of where FHIR is on the Gartner Hype Cycle (see Gartner write up , or Wikipedia ). FHIR Foundation member Wes Rishel ( @wrishel ), who’s a FHIR user, and also was a Gartner Analyst before he retired, graciously made this contribution that I could post here.
I had an email from a company which had a number of really good questions about exposing data through FHIR, so I thought I’d write a post about it rather than just replying directly as it may be of interest to others (and also gives others the opportunity to disagree with me ). The text might also be to a different level of detail.
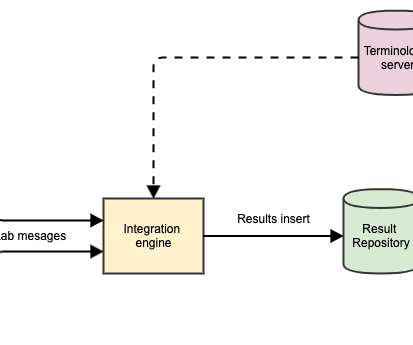
This will be the first post in a short series that considers a very useful interaction – accessing Laboratory data such as blood tests from a repository of data via (of course) a FHIR API. There are 2 core resources, and a number of supporting ones.
At the recent Working Group Meeting in Montreal, I participated in the ‘v2 to FHIR’ stream – focused on how can the HL7 community give advice to implementers about converting v2 messages into FHIR bundles. To actually process (convert to FHIR) a message, click the ‘Convert’ button to the upper right.
As FHIR continues to mature, one of the things we’re seeing is a move away from ‘simple’ data representation Implementation Guides to more complex ones that describe a workflow of some sort. To test this out, I chose a simple use case that uses FHIR notifications to let relatives know when a person is admitted to hospital.
The 23 rd FHIR connectathon in Sydney is almost upon us, and despite the trials and tribulations that the weather has thrown at us, it’s going to be a great event with over 150 people currently scheduled to attend. For myself, I’m going to participate in the FHIR shorthand track. In keeping with the FHIR ethos, the Mitre corp.
So I’ve written an earlier post describing how you can use the excellent HAPI FHIR engine to host your own FHIR server. Of course, you can create your own – or extend the publicly available containers, but the registry makes it trivial to deploy containerized apps (as they are called).
And, of course, you could document this in an Implementation Guide with the appropriate profiles. And finally it was also pointed out that the ConceptMap resource is undergoing significant revision in the next FHIR release (version 5) that will introduce breaking changes. If it’s omitted, then “0” is assumed….
Microsoft took a step to address health data interoperability with Azure API for FHIR in 2019. Patient Unified Health Scoring also provides actionable insights that can help identify potential risks the patients may face and help inform the next-best course of action for that patient.
This years theme is Bringing FHIR into production everywhere! With a serving of AI, of course, because it is 2024, after all. DevDays is my favourite meeting, though unfortunately I don’t get to go this year (though I’m still doing the closing session remotely).
As you probably know, there are a number of ‘conformance’ resources in FHIR that have a unique ‘canonical’ Url that identifies them globally. So how do you accomplish this across different versions of FHIR? So back to FHIR versions. Before we get into that, let’s just address that comment about the ‘major version’.
In part one of this series, we looked at using node-RED to manage notifications using the FHIR Subscription resource for a Use Case where relatives (or other care givers) could be notified when a person is admitted to hospital. This node makes the actual call (a POST) to the FHIR server and validates the resource. User Interface.
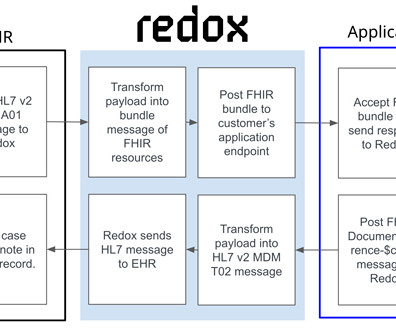
In the first post, I covered how Redox is overcoming current limitations with bulk FHIR. This time, I’ll be discussing our capabilities to translate between HL7 ® v2 and HL7 ® FHIR ® —a reoccurring challenge for many of our customers. However, modern technology shops want everything in FHIR. Let’s dive in. What does HL7 v2 do?
So most of HL7s volunteers are off, urgently making use of their existing infrastructure, or building new solutions in zero time using the standards we’ve already developed – we’ve been building the infrastructure a long time.
To the right of that list is a compressed view of what they should have received – derived from the plan of course Below the Immunization list is the result of the disease analysis described above. You’d want some way to allow the user to set the dates due as well of course. And finally, a list of the API calls needed for this.
Of course that finish line has moved substantially forward. The adoption of FHIR-based standards in Ontario is a notable development. We have achieved all of our wildest dreams from 15 to 20 years ago when we first set down the path of interoperability. We have a long way to go.”
There have been public statements from ONC and to extent from the Sequoia Project that TEFCA will be modernized to computable data – i.e. FHIR data. FHIR has been around for over 10 years so it is worth pondering why it was not incorporated into TEFCA from the start. Of course, the big question is, what is the public benefit?
At the FHIR Connectathon last week I participated in the Questionnaire track and spent most of my time there using – and integration with – the fhirpath lab questionnaire tester tool maintained by Brian Postlethwaite – one of the foundation members of the FHIR community.
At that time, the chats were inspired by advancements in interoperability, including some rather niche healthcare standards discussions, including HL7 v2, HL7 v3, CDA, and eventually FHIR. Of course, if you’re searching for the latest #HITsm chat, you can always find the latest on the #HITsm chat here. Upcoming #HITsm Chat Schedule.
So I’ve just been at the FHIR devdays in Amsterdam which was really interesting (of course – attending a devdays is a ‘must do if possible’ for FHIR implementers). Note also that I’m using the term ’message’ to indicate the input and output – not a Message in the FHIR sense. Create the mapping file (aka ‘map’).
Before we start thinking of the specifics of coding in lab tests, a quick review of coded data in FHIR in general is probably a good idea. This is a common pattern in the FHIR core spec. Looking back at the spec, we see that Observation.code is bound to the LOINC code system with an example binding.
Suppose you have a csv file of data, and you want to load that into a FHIR server. There are a number of ways that you could do that – depending on the nature of the csv file and the capabilities of the FHIR server that you want to update. We could consider the use of a FHIR library – like FHIR.js SNOMED code.
“If #TEFCA is going to invite people in and achieve critical mass, of course we are going to do it.” – Matthew Doyle, Epic on why they decided to join TEFCA. HIMSS23 #HITsm #healthit @CommonWell pic.twitter.com/yLIq8NBs9m — Healthcare IT Today (@hcittoday) April 18, 2023 FHIR APIs are wonderful, but they’re not sufficient on their own.
There’s an extra performance overhead of course – but that’s acceptable to us in this case. Obviously, the call to the Authorization server must be secure, but it does have the advantage that we don’t need to manage keys and the whole decryption process. So let’s implement that. It’s actually quite simple.
I’ve been asked to give a short talk about clinFHIR to a course at Johns Hopkins this month – what it is and what you’d use it for, so to organize my thoughts I decided to write a ‘stock take’ of clinFHIR modules. The idea for clinFHIR started shortly after FHIR started to gain prominence within HL7 – coming up to 10 years ago now.
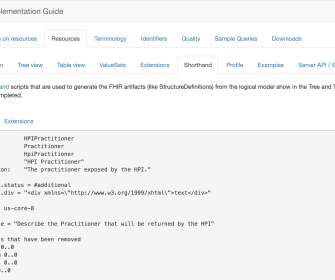
As readers will know, I’m a big fan of FHIR Shorthand as a way of making it much easier to create Implementation Guides and examples in conjunction with the IG publisher. Suppose you are hosting a FHIR API that can create or update Patient resources and you want to say: All patients must include their medical records number (MRN).
One of the things I find myself doing quite often is helping people design FHIR API interfaces. What I find very useful is to create a small set of sample data and save to a generic FHIR server (I use the HAPI server generally, though there are others available these days). Save the resources to the FHIR server.
I’m going to be doing a number of things over the course of the event (a couple of days) – and the days leading up to it. This should be of value to servers implementing an IPS endpoint as well as useful to FHIR beginners as it has a number of useful visualizations. IG’s are the ‘next big thing’ for FHIR.
Enter the world of a standardized API – which is what FHIR specifies. The FHIR specification defines how to search for things in general, and the types of search for each resource in particular – here’s the ones for a Patient. Indeed, this is what allows clinFHIR to select any compliant FHIR server to display patient data from.
Other people contributed – in fact, dropped everything to contribute, all in their own time: Brett Esler gave us free use of his FHIR GP Access library to access the appointment diary for Best Practice, Medical Director, and ZedMed and then worked to improve it for us. In fact, I only did a fraction of the work.
The same question came to me regarding FHIR and http REST. There are two trading partners that have an agreement (Trust Framework) that one will be asking questions using FHIR http REST interfaces of the other party. Conclusion As easy as http REST is, aka FHIR, it is very hard to get security right. Using OAuth is better?
A few of my favorite comments were: “Jim Cramer needs a crash course in FHIR standards” from the wonkier section of peanut gallery. Cramer’s pronouncement led to a tweetstorm where hundreds of tweeters in and outside of health/care talked back and with Cramer. Where is the iPhone listed on Maslow’s hierarchy of human needs?”
The approach I’m taking is to use a ‘vanilla’ FHIR server ( HAPI ) as the actual data repository, with a layer in front of it to manage any specific business functionality I need. This makes sense, as I only want to do this once (after debugging of course) – it’s an administrator function. So that’s enough for the moment.
It helps significantly with the FHIR design. Assuming that the app actually communicates with a FHIR back end (which can be one of the freely available reference servers such as HAPI ), then it validates the resource design (which resources are needed and their profiling) as well as the API’s that are going to be needed.
I mentioned in that post that we didn’t really take a close look at PATCH updates – but a couple of days ago I saw this trail in the FHIR chat which is about a similar project (slightly different requirements) and thought I really should take a closer look at PATCH. Let’s see how that can work (the details are in the FHIR spec of course).
In June this year, there will be the first FHIR DevDays in the United States – in Boston. In fact, last year I attended FHIR DevDays in Amsterdam to guide the clinical track. We talked about using FHIR in clinical scenarios and how tools like clinFHIR support designing the datamodels for these scenarios.
Basically, it’s just a hierarchical model of data – much like you see in any of the core FHIR resource types – with the exception that the model does not have to align with any of the core types. Note that these model types are particular to clinFHIR – they are not ‘official’ FHIR terms. This step does require FHIR knowledge.
We organize all of the trending information in your field so you don't have to. Join 48,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content