This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In this set of posts we’re going to dig into how FHIR supports the use of forms in collecting information. . Forms are ubiquitous in healthcare (and other domains for that matter) so it makes sense that there is some specific support in FHIR for them. The Questionnaire (Q) Is the definition of a form. Simple really.
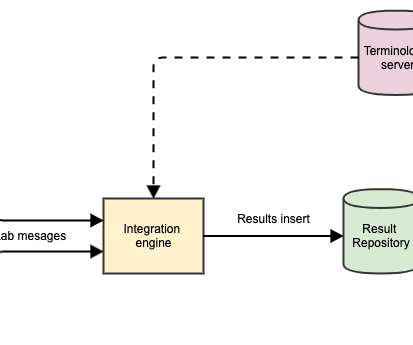
Could be FHIR resources, but more likely a database structure specific to the needs of the lab domain. Well, the simple explanation is that it is a FHIR server (in that it exposes a FHIR interface) that specializes in terminology functionality. FHIR Operation? Above them all is a Terminology Server.
It’s a common thing for implementers to want to do with FHIR: connect to a FHIR server, and make a local copy of the information provided by the server, and then check back occasionally with the server for updates – that is, new resources, or changes to existing resources. (In “I never took X”).
On a forum for FHIR Foundation members, I raised the subject of where FHIR is on the Gartner Hype Cycle (see Gartner write up , or Wikipedia ). FHIR Foundation member Wes Rishel ( @wrishel ), who’s a FHIR user, and also was a Gartner Analyst before he retired, graciously made this contribution that I could post here.
Users are grouped into "clearances" (aka roles); this might be a FHIR PractitionerRole, CareTeam, RelatedPerson, and Group; but might be something non-FHIR (aka OAuth, LDAP, etc). The SLS must understand FHIR. Policies indicate what "clearance" (aka roles) have access to each data "classification".
Looking at the proposal for the next version of FHIR (R5) it is multiple, but we can’t use that yet. The ‘plan definition’ extension specifies the url and value explicitly, while the ‘disease covered’ uses a named extension. These were: planDefinitionUrl. diseaseCovered.
At the recent Working Group Meeting in Montreal, I participated in the ‘v2 to FHIR’ stream – focused on how can the HL7 community give advice to implementers about converting v2 messages into FHIR bundles. To actually process (convert to FHIR) a message, click the ‘Convert’ button to the upper right.
I will be giving a face-to-face tutorial on the topic of "IHE on FHIR" at both HL7 Workgroup meeting in Cologne, May 12-18 FHIR Dev Days in Boston, June 19-21 So, if you are in Europe, sign up for the tutorial at HL7 workgroup meeting. If you are in the USA, sign up for the tutorial at FHIR Dev Days.
Integrating the Healthcare Enterprise (IHE) has been busy creating Profiles that leverage the new and exciting FHIR specification. IHE publishes their profiles on [link] IHE subset of Profile on FHIR can be found on the IHE wiki FHIR list An IHE Profile is equivalent to a FHIR Implementation Guide.
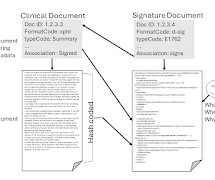
The IPS is a Document, and there is a definition for this document using CDA and using FHIR. The FHIR Document is the one most are interested in. At the technical level, they are equivalent, and they meet the same abstract definition defined by ISO/CEN. But FHIR is the hot new standard, so everyone wants to use it.
I was trying to remember how to represent family relationships in FHIR – to record that one person is related to another, maybe a mother / daughter relationship, assuming that each person is already represented by a Patient resource. The following are the overall steps I followed. Install sushi. See the online instructions.
So a little while back I wrote about an app I developed during the WGM Connectathon to send an HL7 v2 message to a converter app, and display the response (a FHIR Bundle ) in a number of visualizations after validating it using the community supplied validation tool (actually, exposed by the reference servers via the $validate operation).
The FHIR R4 ballot is out (see announcement), and I’d like to draw attention to one part of FHIR that we’ve been working hard on during the preparation of R4: Patterns. In FHIR, we made a specific decision to be as specific as we can get away with. FHIR Patterns. Specific vs General.
As you probably know, there are a number of ‘conformance’ resources in FHIR that have a unique ‘canonical’ Url that identifies them globally. This SHALL be a URL, SHOULD be globally unique, and SHOULD be an address at which this structure definition is (or will be) published. So back to FHIR versions. For ValueSet.
The 23 rd FHIR connectathon in Sydney is almost upon us, and despite the trials and tribulations that the weather has thrown at us, it’s going to be a great event with over 150 people currently scheduled to attend. For myself, I’m going to participate in the FHIR shorthand track. In keeping with the FHIR ethos, the Mitre corp.
This conversion enabled better and more comprehensive definition of the Provenance linkage between the derived FHIR clinical Resources and the source documents from the HIE. This Provenance definition is now in mXDE along with examples and requirements CapabilityStatement.
So I’ve written an earlier post describing how you can use the excellent HAPI FHIR engine to host your own FHIR server. Let’s take the simplest case – we just want to set up a FHIR server on your local machine. The following command will do the trick.
A really short post to record how to download the core extensions in the spec (This came up in a FHIR Chat today). This is particularly useful if you are setting up your own FHIR server and want to pre-load them with the code definitions in the spec. They can be found at: [link].
This years theme is Bringing FHIR into production everywhere! That’s an awesome spread of content that definitely makes it worth attending. DevDays is my favourite meeting, though unfortunately I don’t get to go this year (though I’m still doing the closing session remotely).
I work with the team on the transition to FHIR. The details on my speaking engagement at virtual HIMSS are that it is about the opportunity that is coming (not yet here) enabled by FHIR and the CarePlan resource in FHIR. It is also the likely solution you would have needed to use to fly to Vegas -- In AUGUST!!!
We spent a bit of time in the last post describing why we want to have data coded, how FHIR supports coded data – especially the external terminologies where the concepts are defined – and described some of the RESTful API calls that we could make to retrieve specific Observations and DiagnosticReports from the repository.
Last week we held our first New Zealand ‘ Clinicians on FHIR ‘ seminar at the HINZ conference in Rotorua. This uses FHIR Logical Models – so an understanding of FHIR datatypes is desirable (though not mandatory). Finally the actual FHIR Conformance artifacts can be generated.
FHIR defines a Questionnaire resource that specifies a set of questions for a user, along with a QuestionnaireResponse resource to capture their response. This extension says that the form filler takes a parameter which is a FHIR Patient resource. A variable has a name, and a value which is a list of resources or FHIR types.
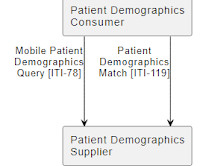
IHE ITI has a set of profiles on FHIR existing in Trial Implementation today. These were written against FHIR DSTU2. This profile does rely on creative systems engineering to decompose the documents into the FHIR resources. This might leverage CDA-on-FHIR, or some other methodology. This methodology is not specified.
So I’ve just been at the FHIR devdays in Amsterdam which was really interesting (of course – attending a devdays is a ‘must do if possible’ for FHIR implementers). Note also that I’m using the term ’message’ to indicate the input and output – not a Message in the FHIR sense. The firely approach uses 2 operations.
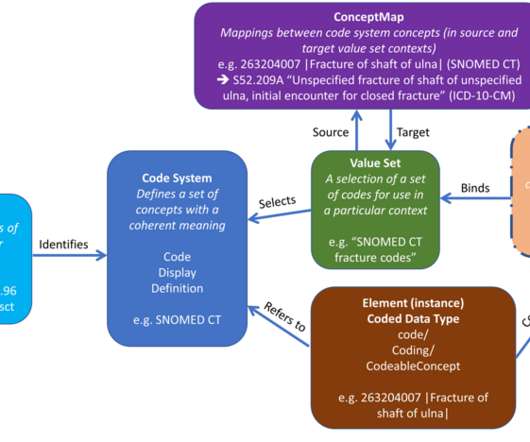
FHIR defines an extension to use to state the the value set a Coding was taken from: "coding": [{ "system": "[link] "code": "39065001", "display": "Burn of ear", "extension" : [{ "url" : "[link]. from the FHIR spec ). btw, If we could go get the definition of [link] we could validate the code against that too.
Much discussion around consent (Privacy) in HL7 FHIR. FHIR should focus on only what systems do today, not what we want them to do. FHIR should put into common extensions those things that we want them to do (e.g. If we can agree on this, then the role of FHIR in capturing consent would be immensely clearer.
I have been asked quite often to explain how to secure FHIR. The basics of Security for FHIR are written up on the FHIR Specification. Don’t worry about security The first answer is the one I give to those in HL7 that are working on developing FHIR, or just getting their feet wet learning FHIR. Not too big.
Something supported by IHE Document Sharing (XDS/XDR/XDM/XCA/MHD), something enabled and using #FHIR. I use "document", with a lower-case "d", when I am referring to an object that meets the Internet's definition of a document. Everything else in the Bundle is just FHIR Resources. When is a Document a Document?
Before we start thinking of the specifics of coding in lab tests, a quick review of coded data in FHIR in general is probably a good idea. It can represent an external terminology such as LOINC or SNOMED, or can contain the actual definition of the concepts directly. This is a common pattern in the FHIR core spec.
How does one put a FHIR Document into XDS? How does one find a FHIR Document in XDS? Both of these might still be needed for FHIR Documents. FHIR is more popularly known for the access model using http REST. FHIR has a Document model. There is also a workgroup creating transforms from/to CDA -- CDA on FHIR.
So we’ve talked about how to represent an immunization program both in the abstract (the overall definition of a national plan) and the specific (the plan applied to an individual). In addition, we discussed how to submit the actual administrations to the registry.
There is renewed discussion, much like back in January, around the need to go beyond testing just the FHIR Resource 'interoperability'. A 'system' in the broadest of definitions. This reference system needs to pick a minimum-useful set of FHIR resource centric workflows. This is more than just a selection of FHIR Resources.
This is an update of what is going on in Security and Privacy in, and around, the FHIR specification. This is an update of what is going on in Security and Privacy in, and around, the FHIR specification. GDPR driven activities: The Security WG has done an assessment of FHIR in the context of GDPR.
Rene asked for an outline of Security topics for FHIR for an upcoming tutorial he is giving. The easy answer is go read all my blog articles under the #FHIR topic The second easy answer is to point at the FHIR security pages. There are efforts underway to create a Privacy Consent Directive modeled in FHIR.
This means that when I attended the FHIR Connectathon 14, prior to the HL7 Workgroup Meeting in San Antonio TX , I was shocked to experience the new FHIR Connectathon. The others from the FHIR core-team have seen the changes over-time, so the transition is not as shocking as it was for me. FHIR has matured, it is growing up.
This is actually part of a project I’ve been working on for a little while – learning FHIR with clinFHIR – so it’s a perfect time to be doing it. The idea for clinFHIR started shortly after FHIR started to gain prominence within HL7 – coming up to 10 years ago now.
Bulk Data Access The addition of a Bulk Data Access in #FHIR was a hot topic at the San Diego workgroup meeting. Which is not a definition of a use-case. I have addressed this topic in FHIR before, FHIR does not need a deidentify=true parameter. This effort would best be done as the FHIR resources approach maturity.
I have been pushing IHE to add FHIR conformance resources to their publication mechanism. I now have published the full set of FHIR conformance resources for PDQm and MHD profiles. FHIR conformance resources are available to carry programatically the constraints that historically IHE has written narratively into an IHE Profile.
Updated: Vadim Peretokin advises on the FHIR chat : You're better off in the world if you know about this stuff though. Specifically, with regard to the java reference implementation, it has always ignored DTD definitions, so is immune. Any newly released versions will change to stop ignored DTD definitions, and report an error.
Example Standards: FHIR + v2 (from HL7 ) Snomed CT LOINC DICOM (from NEMA ) etc (there’s 100+ organizations creating platform standards). Thing is, that’s what FHIR does too, and it’s very definitely a platform standard. They define how things can work. There’s lots of organizations working in this space.
This winter quarter will be a lighter load, recognizing the holidays: Patient Scheduling, prospective look at FHIR R5/6, and evaluating impact of Gender Harmony. The Non-Patient File Sharing (NPFS) Profile defines how to share non-patient files such as clinical workflow definitions, domain policies, and stylesheets.
Great move for HISPS to use FHIR to update the directory versus batch file updates. My favorite piece of this is the move to FHIR updates versus the current batch file updates. Definitely a superior solution, but also is going to take some development work by vendors to switch to this new approach.
We should definitely have one eye on the horizon, in a world where all data in healthcare is freely flowing between all parties who need access. However, rather than jump from fax all the way to electronic data exchange through FHIR or APIs, Turicchi suggests that we should leverage the inherent network effect that fax still enjoys. “We
We organize all of the trending information in your field so you don't have to. Join 48,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content