This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Most of the data that we are looking to share is highly sensitive healthinformation, the kind of information that cybercriminals love to hold for ransom. A clear definition of what is considered sensitive information subject to such rules and directives has not yet been established.
Users are grouped into "clearances" (aka roles); this might be a FHIR PractitionerRole, CareTeam, RelatedPerson, and Group; but might be something non-FHIR (aka OAuth, LDAP, etc). A good example is Observation.category code of 'vital-signs' -- indicates vital signs that are normal healthinformation of no stigmatizing sensitivity.
The first is the ability to exchange a list of health data locations, which enables Record Locator Services to interoperate with consumers wishing to discover the location of patient records within a healthinformation exchange. This Provenance definition is now in mXDE along with examples and requirements CapabilityStatement.
.” The OECD report assesses digital health maturity across 22 countries: in addition to the U.S., The definition of “digital health” has not been set in stone (don’t we know it!) In health care, we have a plethora of standards for linking healthinformation from disparate data sets.
How does one put a FHIR Document into XDS? How does one find a FHIR Document in XDS? To learn more on Document Sharing, start here: Eating an Elephant -- How to approach IHE documentation on HealthInformation Exchange (HIE) So the Document Sharing family is a Content Agnostic mechanism for sharing Patient specific Documents.
This is an update of what is going on in Security and Privacy in, and around, the FHIR specification. This is an update of what is going on in Security and Privacy in, and around, the FHIR specification. GDPR driven activities: The Security WG has done an assessment of FHIR in the context of GDPR.
This winter quarter will be a lighter load, recognizing the holidays: Patient Scheduling, prospective look at FHIR R5/6, and evaluating impact of Gender Harmony. The Non-Patient File Sharing (NPFS) Profile defines how to share non-patient files such as clinical workflow definitions, domain policies, and stylesheets.
Etienne Boshoff, Managing Director at EHR Enhancify Healthcare interoperability is advancing through the adoption of Electronic Health Records (EHRs), standardized APIs like FHIR, and emerging technologies such as blockchain. These challenges can be effectively addressed through several strategies.
But the administrative costs for providers to share this information keep escalating. The healthcare industry’s steady progress toward interoperability and healthinformation exchange promises to improve data exchange to address these challenges. Automated chart retrieval is performed at scale, leveraging modern HL7 FHIR APIs.
In the past two weeks I have been in large audience discussions where there is a very different kind of topic being discussed around HealthInformation Technology. These things have been greatly supported by current HealthInformation Exchange (IHE Document Sharing using XDS/XCPD/XCA). It is not explicitly said that way.
On Friday last week, an article by Wendy John was published by Wild Health , in which I’m quoted as saying, regarding the My Health Record and the Strengthening Medicare Taskforce report : FHIR guru Grahame Grieve has advocated for interoperability standards in healthcare for over two decades.
Lyniate , a global leader in healthcare data interoperability, and CareCom , a leader in healthcare terminology management solutions including HealthTerm® and CareIndexing®, have entered into a definitive merger agreement.
The recommendation I give here is restricted to the gross level: for Document Sharing at the XDS/XCA/DocumentReference metadata level; for FHIR REST at the returned Bundle.meta.security level, but not on each Resource in the Bundle; and for CDA at the CDA header, but not on each element. Available from the FHIR specification for easy reading.
Micky is the president and CEO of the Massachusetts eHealth Collaborative , a non-profit health IT advisory and clinical data analytics company ( @MAeHC_org ), and is a nationally recognized leader in healthinformation technology. Organizations that have a trust relationship can exchange data on a bulk basis (e.g.
Micky is the president and CEO of the Massachusetts eHealth Collaborative , a non-profit health IT advisory and clinical data analytics company ( @MAeHC_org ), and is a nationally recognized leader in healthinformation technology. Organizations that have a trust relationship can exchange data on a bulk basis (e.g.
Micky is the president and CEO of the Massachusetts eHealth Collaborative , a non-profit health IT advisory and clinical data analytics company ( @MAeHC_org ), and is a nationally recognized leader in healthinformation technology. Organizations that have a trust relationship can exchange data on a bulk basis (e.g.
Micky is the president and CEO of the Massachusetts eHealth Collaborative , a non-profit health IT advisory and clinical data analytics company ( @MAeHC_org ), and is a nationally recognized leader in healthinformation technology. After that, you can listen on demand (See podcast information below.)
Micky is the president and CEO of the Massachusetts eHealth Collaborative , a non-profit health IT advisory and clinical data analytics company ( @MAeHC_org ), and is a nationally recognized leader in healthinformation technology. After that, you can listen on demand (See podcast information below.)
Micky is the president and CEO of the Massachusetts eHealth Collaborative , a non-profit health IT advisory and clinical data analytics company ( @MAeHC_org ), and is a nationally recognized leader in healthinformation technology. After that, you can listen on demand (See podcast information below.)
Add an ITI-65 FHIR Documents Publish option with support in ITI-65 to include a FHIR Document Bundle as an alternative to Binary. Converted from PDF to a FHIR IG. Very focused on #FHIR, but also enabled by existing and successful XDS/XCA HealthInformation Exchange. was released.
This scenario has become the standard in today’s virtual health programs. But this kind of integration isn’t complete and it definitely doesn’t enable interoperability. The data exchange you expected – and need – isn’t an option. The Danger of Integration Limitations. So here’s some good news.
Some examples where BPPC are used: Connecticut HIE: For release of Privileged Care information, a consent document SHALL be registered with HITE-CT in the form of a BPPC conformant document using the Opt-in for Legally Protected Data (ALL) policy. This article is all about IHE Document Sharing, and not about FHIR. 38571.2.1.3.2
What we’re seeing is more companies leverage things like wearable data, glucose monitor data to learn more about users to improve both preventative health and care for chronic conditions throughout the care journey.
IHE FormatCodes are mandatory In Wisconsin we have Interoperability What is MHD beyond XDS-on-FHIR? This local processing might further eliminate unnecessary entries, might sort the results, might put emphasis on some entries because of specific metadata entries. This local processing might be automated algorithm, or might involve a human.
The Patient is NOT the center of existing HealthInformation Exchange. Yet, the HealthInformation Exchange exists for the sole purpose of treating that Patient. The HealthInformation Exchanges today have an existing Architecture. When I 'used' I also mean the broadest definition. What did they get?
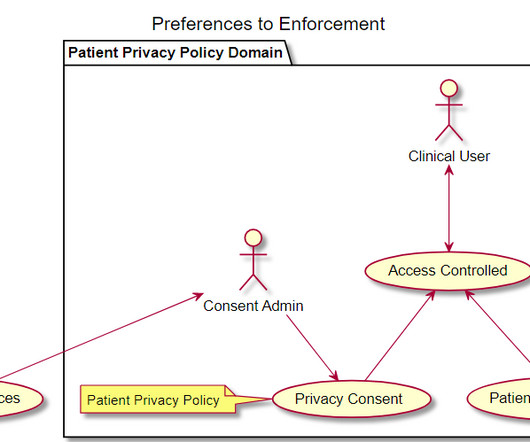
Given XDS and XCA interactions that are often used in an HealthInformation Exchange (HIE), or a National HealthInformation Exchange (NHIE); there is no standards/profiled way to enable a point-of-care consent gathering workflow. So today, if Consent is not already captured, and needed, then data access is blocked.
As part of my advisory position on SHIFT Shift (formerly Protecting Privacy to Promote Interoperability PP2PI) was founded in 2018 and formalized in 2020 with a mission to advance safe, equitable, and patient-empowered sharing of healthinformation. It should be by the time they finish their comments.
This scenario has become the standard in today’s virtual health programs. But this kind of integration isn’t complete and it definitely doesn’t enable interoperability. The data exchange you expected – and need – isn’t an option. The Danger of Integration Limitations. So here’s some good news.
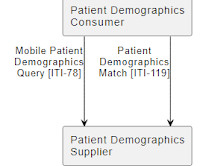
Leslie noted that patient matching is a significant issue for her organization’s constituency – health care organizations’ CIOs – both for immediate patient care reasons and because it is difficult to have meaningful conversations about interoperability without the means to definitively identify patients.
Leslie noted that patient matching is a significant issue for her organization’s constituency – health care organizations’ CIOs – both for immediate patient care reasons and because it is difficult to have meaningful conversations about interoperability without the means to definitively identify patients.
Leslie noted that patient matching is a significant issue for her organization’s constituency – health care organizations’ CIOs – both for immediate patient care reasons and because it is difficult to have meaningful conversations about interoperability without the means to definitively identify patients.
Leslie noted that patient matching is a significant issue for her organization’s constituency – health care organizations’ CIOs – both for immediate patient care reasons and because it is difficult to have meaningful conversations about interoperability without the means to definitively identify patients.
Leslie noted that patient matching is a significant issue for her organization’s constituency – health care organizations’ CIOs – both for immediate patient care reasons and because it is difficult to have meaningful conversations about interoperability without the means to definitively identify patients.
Leslie noted that patient matching is a significant issue for her organization’s constituency – health care organizations’ CIOs – both for immediate patient care reasons and because it is difficult to have meaningful conversations about interoperability without the means to definitively identify patients.
We can't change Healthcare by writing very complex standards like the current FHIR ConsentDirective , which is fundamentally a " Contract " resource. First I recommend that FHIR make ConsentDirective a resource rather than just profiles of Contract. But we can't go from one view to the other without taking some small steps.
authorized for wide distribution – like an emergency-data-set, or for dietary use-cases "L", because the content is not medical, or has been de-identified "U", because the content is not specific to an individual and is public This is right out of the definition of the vocabulary values 2.16.840.1.113883.5.25 See FHIR Demonstration of DS4P.
Second, Redox transforms the myriad of data specifications in use today—such as FHIR, HL7v2, CDA/CCD, X12, XML, custom CSVs—into a standard set of JSON data models. Redox has worked with the major EHR vendors, CRMs, and HealthInformation Exchanges. Further, Redox ensures that data is normalized to standard value sets.
We are very pro consumers getting their healthinformation. We also do tens of millions of doctor requests for information for continuity of care and things like that, for which we don’t charge, of course. We lean in heavily on the Argonaut system, which is HL7 standards-based FHIR communication.
Grahame Grieve is a principal with Health Intersections of Melbourne, Australia and was the architect-developer of HL7’s Fast Healthcare Interoperability Resources (FHIR, pronounced “fire”) specification that allows EHRs to exchange information. Was it weird to see FHIR as the only universal topic of HIMSS19?
. – February 26, 2020 – GlobalMed, a leading provider of virtual health solutions, today announced that it will showcase integration enhancements to its virtual health platform eNcounter®, introduce a backpack telehealth exam station, and offer a lighter, more affordable exam camera at HIMSS20, March 9-13 in Orlando, FL.
EHR companies are building strong partnerships with Avizia to leverage robust API libraries, software development kits (SDKs) and integration “gateways” to quickly deliver cutting edge virtual health solutions to their customers. “We Often, a browser and web camera are all that are needed. Read More.
We organize all of the trending information in your field so you don't have to. Join 48,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content