This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In the USA and elsewhere, there are Document Sharing based HealthInformation Exchanges. The solution is to leverage this existing solution, and just add FHIR. The PUSH model is used to convey information to a specified recipient. Just add FHIRFHIR is a content format. These metadata are well talked about.
Four years ago, we reached a milestone when leaders from three federal entities announced landmark healthcare technology regulations centered around a clinical data-sharing standard called Fast Healthcare Interoperability Resource, or FHIR (pronounced “fire”). Rate limiting is not inherent to the FHIR standards.
I already have one proposal for the transition from the current Federated HealthInformation Exchange to supporting FHIR, that is based on a transition from CDA to FHIR-Documents. Federated FHIR Resource Servers In this article I am going to add another step to the smooth transition. I will get to those later.
We talk a lot about sharing data and how it will improve patient outcomes and interoperability, but do we talk enough about how to do it safely? Most of the data that we are looking to share is highly sensitive healthinformation, the kind of information that cybercriminals love to hold for ransom.
One of the most significant applications of healthcare information technology is the exchange of healthinformation among disparate clinical information systems and otherwise unaffiliated care providers. The HealthInformation Exchange model presented is an Infrastructure, it is not constraining the content.
Most use of FHIR today is as an API to an organizations healthinformation (EHR). However what is being asked latey is how does one scale FHIR to a nation. I have plenty of articles on how a Nationwide HealthInformation Exchange (HIE) could be built with the IHE XD* family of profiles.
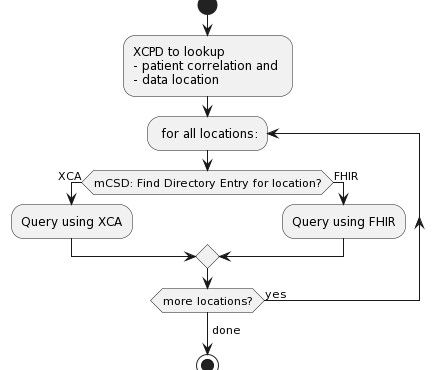
The first is the ability to exchange a list of health data locations, which enables Record Locator Services to interoperate with consumers wishing to discover the location of patient records within a healthinformation exchange. Details on who IHE is and how to engage are available on their web site.
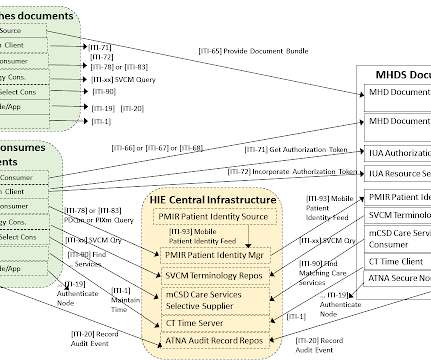
This profile shows how to build a Document Sharing Exchange using IHE profiled FHIR® standard, rather than the legacy IHE profiles that is dominated by XDS and HL7® v2. The MHDS Profile specifies how a collection of IHE profiles can be used by communities for exchanging healthinformation. 3 - Section 4.0
But the administrative costs for providers to share this information keep escalating. The healthcare industry’s steady progress toward interoperability and healthinformation exchange promises to improve data exchange to address these challenges. Here is one example of how payer exchange is being automated today.
The FHIR security tag `VIP` is used to indicate that a patient's healthinformation is considered to be highly confidential and requires heightened security measures. To use the VIP security tag, simply add it to the security tag of any FHIR resource that contains the patient's healthinformation.
TEFCA outlines a common set of principles, terms, and conditions to enable the nationwide exchange of healthinformation across disparate healthinformation networks (HINs). We applaud the hard work that the ONC, CMS, The Sequoia Project, and the Qualified HealthInformation Exchanges (QHINs) have done to bring it live.
I have covered the vision of Data Segmentation for Privacy (DS4P) concept, and outline how a Security Labeling Service (SLS) would enable this grandiose vision of DS4P. However, there are stepping stones: The following is a slightly update on an article I wrote in July 2015 on how to set the confidentialityCode. for "_confidentiality".
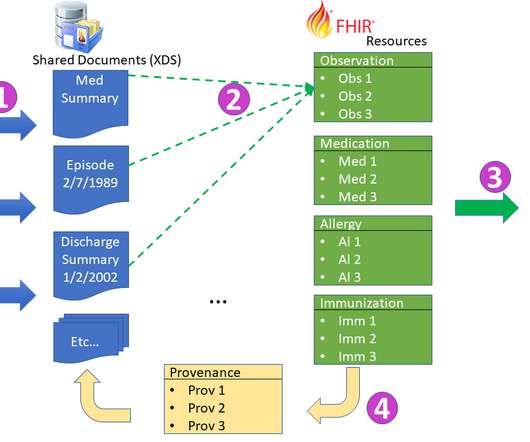
How does one put a FHIR Document into XDS? How does one find a FHIR Document in XDS? Both of these might still be needed for FHIR Documents. FHIR is more popularly known for the access model using http REST. FHIR has a Document model. If I have a FHIR Document, how would I publish that into XDS?
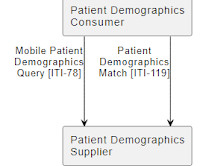
IHE has created a FHIR based Patient identity management system for healthinformation exchanges. Added to this is a set of requirements and expectations around how Merging (Link and UnLink) are to be implemented. It is possible that a formal Merge will be supported, but in FHIR a Merge comes with some downsides.
The ONC Cures Act APIs and the companion CMS Access APIs all require these modern FHIR-based technologies and are fundamentally designed to grow a vibrant digital health economy providing choice and value to consumers. These API protocols are known and used by hundreds of thousands of developers.
Healthcare providers will be facing IT pressures: how to enable more people to make use of more sensitive data in a secure and compliant way, while also being economically efficient. In 2023, health IT vendors will continue to work to maintain compliance as part of new regulatory requirements related to the 21st Century Cures Act.
This winter quarter will be a lighter load, recognizing the holidays: Patient Scheduling, prospective look at FHIR R5/6, and evaluating impact of Gender Harmony. The Non-Patient File Sharing (NPFS) Profile defines how to share non-patient files such as clinical workflow definitions, domain policies, and stylesheets.
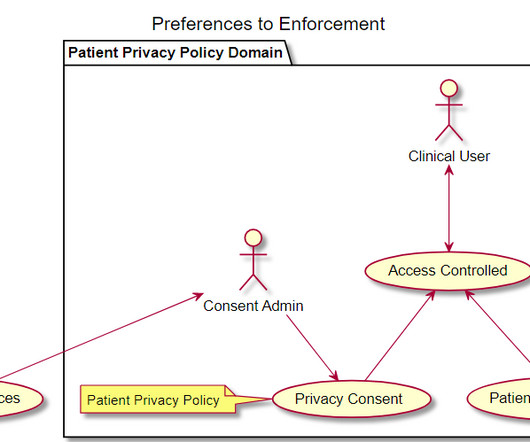
The topic is Patient Privacy Consent; the discussion is if this should be modeled as a core FHIR Resource, or as a core FHIR Profile upon the Contract Resource. With the CBCC workgroup focusing on how to capture a Patient Privacy Consent, and the Security workgroup focusing on how to enforce this.
The Argonaut Project is a collaborative effort between the healthcare industry and the technology industry to develop and implement standards for exchanging electronic healthinformation (EHI). The Argonaut Project focuses on the development and implementation of FHIR, a standard for exchanging healthcare data.
Reminder that I am discussing how to scale Patient Centric Exchanges given the following challenges: How do I find all the data holders for a given Patient? How do I prove I am secure and trustworthy? How do I get data and assure it is authentic? The overall models between XD* and FHIR are the same.
About NYeC New York eHealth Collaborative (NYeC) is a not-for-profit organization working in partnership with the New York State Department of Health to improve healthcare by collaboratively leading, connecting, and integrating healthinformation exchange across the State.
It takes time to write a programming library that can extract each field from an EHR and present it to an outside program, even given the modern FHIR standard (itself complex and evolving). These observers point out that patient data is extraordinarily large and complex. The API gap is, Bari says, “when regulation meets reality.”
DirectTrust is adopting a FHIR-based approach to making updates to its provider directory , which contains more than 1 million addresses. DirectTrust President and CEO Scott Stuewe talked to John about what this project entails and how it will make a difference for information sharing.
Available from the FHIR specification for easy reading. link] How to determine what the value should be? See FHIR Demonstration of DS4P. "M", because the content is less sensitive than normal, but still medical. for "_confidentiality". I don't disagree that this is a hard thing to determine.
This became possible thanks to electronic health records, telemedicine, and cloud solutions. Let’s discuss how to tackle them and explore the IT solutions essential for modern healthcare institutions. To seamlessly obtain information from various systems, healthcare data exchange standards are essential.
This IHE-Profile (aka Implementation Guide) provides guidance on how to implement the sharing of terminology ValueSets, CodeSystems, and ConceptMaps. This IHE-Profile (aka Implementation Guide) provides for a HealthInformation Exchange Community to cooperate on a golden (master) identity for the Patients.
Like most of us, Andy Oram has a health insurance card in his wallet. Here’s what he learned about SMART Health, FHIR, registries, EHR integrations, and other technology that could support digital insurance cards in the not-too-distant future. Read more… Why the Future is Bright for HealthInformation Management.
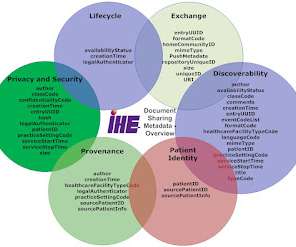
Where the combined list is available in FHIR as a ValueSet of FormatCodes (updated in current build ) Important background :: Eating an Elephant -- How to approach IHE documentation on HealthInformation Exchange (HIE) and Healthcare Metadata The FormatCode is there to differentiate 'technical format'. is one FormatCode.
In the past two weeks I have been in large audience discussions where there is a very different kind of topic being discussed around HealthInformation Technology. The topic is about a vision of how things could/should be at the point of care because of successful interoperability. It is not explicitly said that way.
IHE is currently working on a "Handbook" intended to instruct an XDS Affinity Domain, or Community (XCA), or MHD community on how to structure their requirements on metadata. Later I explain how to deal with this fragility. IHE FormatCodes are mandatory In Wisconsin we have Interoperability What is MHD beyond XDS-on-FHIR?
Some examples where BPPC are used: Connecticut HIE: For release of Privileged Care information, a consent document SHALL be registered with HITE-CT in the form of a BPPC conformant document using the Opt-in for Legally Protected Data (ALL) policy. This article is all about IHE Document Sharing, and not about FHIR. 38571.2.1.3.2
As part of my advisory position on SHIFT Shift (formerly Protecting Privacy to Promote Interoperability PP2PI) was founded in 2018 and formalized in 2020 with a mission to advance safe, equitable, and patient-empowered sharing of healthinformation. Why do I express this?
Given XDS and XCA interactions that are often used in an HealthInformation Exchange (HIE), or a National HealthInformation Exchange (NHIE); there is no standards/profiled way to enable a point-of-care consent gathering workflow. So today, if Consent is not already captured, and needed, then data access is blocked.
As proof, FHIR Documents will re-open this discussion. Especially with the CDA-on-FHIR efforts. Given a HealthInformation Exchange, or Nationwide HealthInformation Exchange, there will be a variety of capabilities and use-cases for the hundreds-thousands of various Document Consumers. are laying around.
You’ll collaborate closely with others on the various technologies of our healthinformation exchange platform to implement software solutions. HOW TO APPLY: Please email a copy of your cover letter and resume to HR@transformsso.ca. We welcome and appreciate your interest in our organization. Visit our website to learn more!
Teladoc Health and Ovation Medical are among the organizations that will utilize these new capabilities. Meditech will use Google Health's technologies to build a longitudinal health data output that combines data from multiple sources using standard FHIR format. Virtual care. Map route optimization.
Here are some specific reflections: FHIR adoption: We missed the mark on our HL7® Fast Healthcare Interoperability Resources (FHIR®) growth prediction. It certainly is growing, but FHIR has not picked up the steam we had hoped for in 2023. We reflected on that in our recap of 2023 FHIR DevDays. Sadly, he was wrong.
If this looks like a position that would interest you, check out the full details for the job and how to apply. As always, you can search our Health IT job board for a variety of jobs from leading companies in the industry. Looks like a great opportunity for those with experience with analyzing EHR applications!
Algorithms based on biased data can lead to inaccurate diagnoses, predictions, and actions that can further marginalize vulnerable populations, fuel racism, and drive worse health and financial outcomes. For example, the CMS-0057-P proposed rule requires the use of FHIR APIs and essentially builds upon previous regulations.
For healthinformation technology (HIT) and electronic health record (EHR) vendors, new regulations that promote interoperability and transparency for PA workflows are an opportunity to significantly improve the experience for providers and the patients they serve.
We organize all of the trending information in your field so you don't have to. Join 48,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content